

Trauma-Induced Nanohydroxyapatite Deposition in Skeletal Muscle is Sufficient to Drive Heterotopic Ossification
- PMID: 30515544
- PMCID: PMC6437294
- DOI: 10.1007/s00223-018-0502-5
Trauma-Induced Nanohydroxyapatite Deposition in Skeletal Muscle is Sufficient to Drive Heterotopic Ossification
Abstract
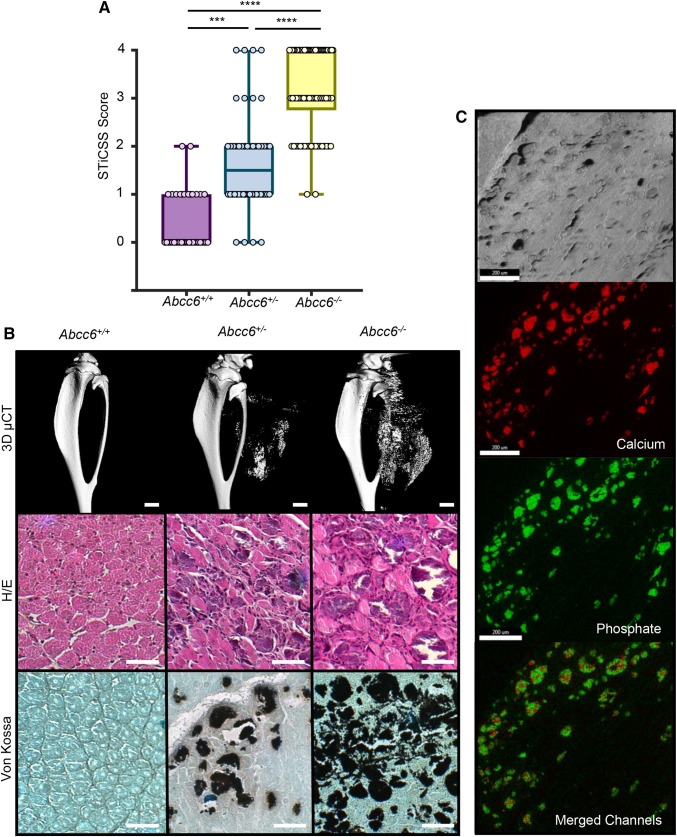
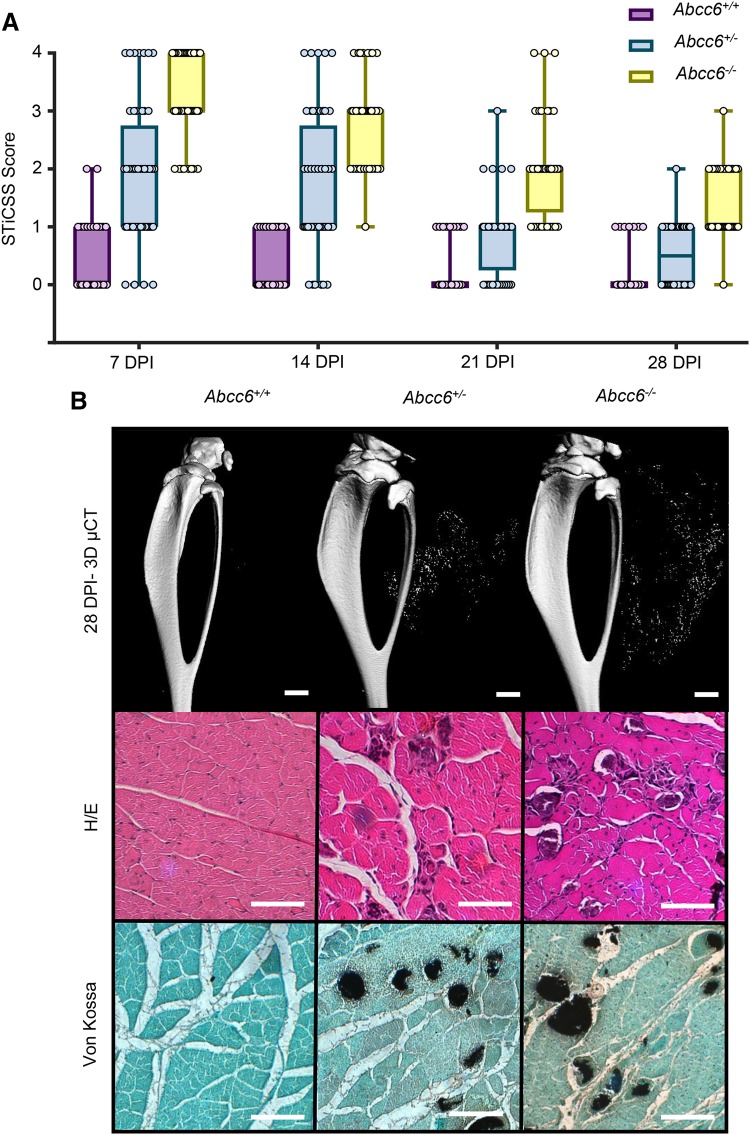
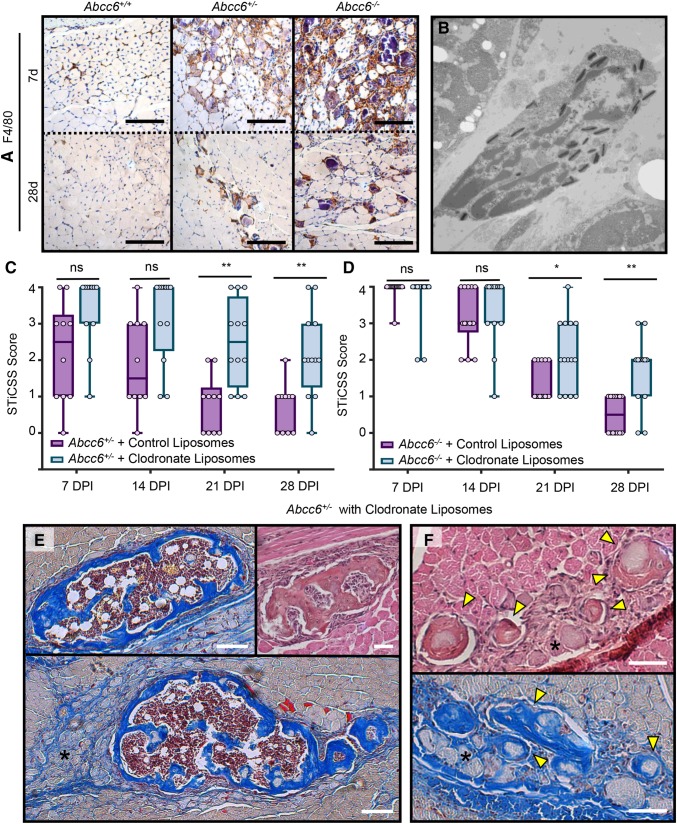
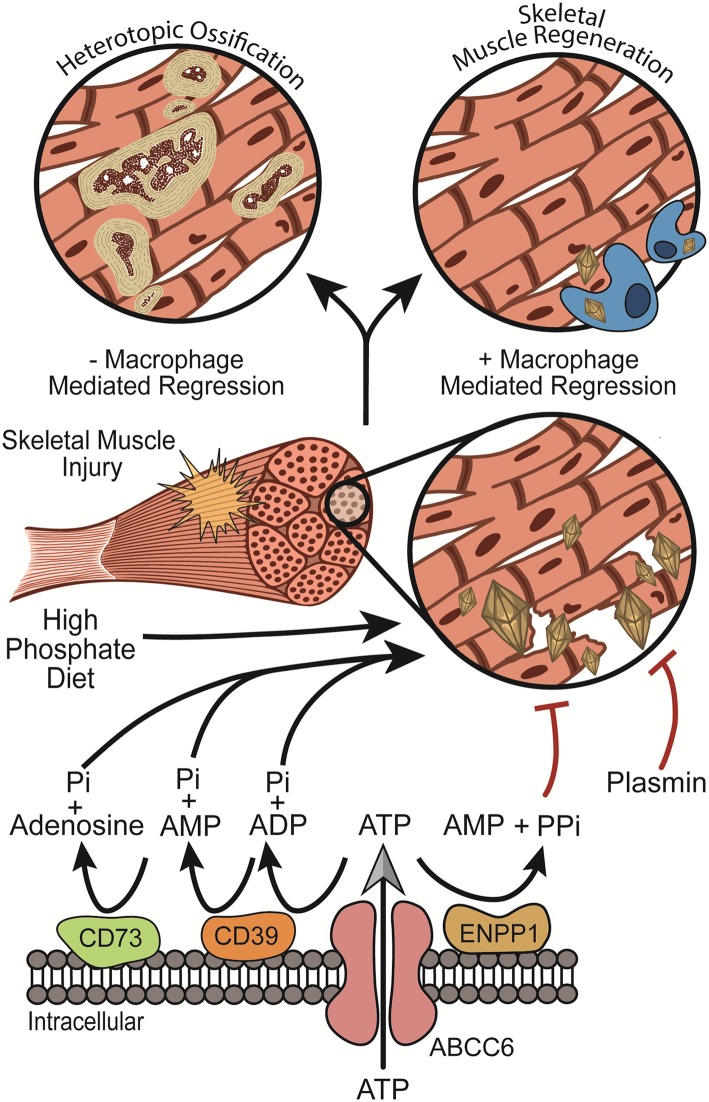
Heterotopic ossification (HO), or the pathologic formation of bone within soft tissues, is a significant complication following severe injuries as it impairs joint motion and function leading to loss of the ability to perform activities of daily living and pain. While soft tissue injury is a prerequisite of developing HO, the exact molecular pathology leading to trauma-induced HO remains unknown. Through prior investigations aimed at identifying the causative factors of HO, it has been suggested that additional predisposing factors that favor ossification within the injured soft tissues environment are required. Considering that chondrocytes and osteoblasts initiate physiologic bone formation by depositing nanohydroxyapatite crystal into their extracellular environment, we investigated the hypothesis that deposition of nanohydroxyapatite within damaged skeletal muscle is likewise sufficient to predispose skeletal muscle to HO. Using a murine model genetically predisposed to nanohydroxyapatite deposition (ABCC6-deficient mice), we observed that following a focal muscle injury, nanohydroxyapatite was robustly deposited in a gene-dependent manner, yet resolved via macrophage-mediated regression over 28 days post injury. However, if macrophage-mediated regression was inhibited, we observed persistent nanohydroxyapatite that was sufficient to drive the formation of HO in 4/5 mice examined. Together, these results revealed a new paradigm by suggesting the persistent nanohydroxyapatite, referred to clinically as dystrophic calcification, and HO may be stages of a pathologic continuum, and not discrete events. As such, if confirmed clinically, these findings support the use of early therapeutic interventions aimed at preventing nanohydroxyapatite as a strategy to evade HO formation.
Keywords: Abcc6; Dystrophic calcification; Heterotopic ossification; Nanohydroxyapatite; Skeletal muscle injury.
Conflict of interest statement
Conflict of interest
Jonathan G. Schoenecker is a member of the education advisory board at OrthoPediatrics and receives research funding from OrthoPediatrics and research support from IONIS Pharmaceuticals. Jonathan G. Schoenecker receives research support from PXE International. Stephanie N. Moore-Lotridge, Qiaoli Li, Breanne H. Y. Gibson, Joseph T. Martin, Gregory D. Hawley, Thomas H. Arnold, Masanori Saito, Sami Tannouri, Herbert S. Schwartz, Richard J. Gumina, Justin M.M. Cates, Jouni Uitto, and Jonathan G. Schoenecker have declared that no conflict of interest exists.
Human and Animal Rights and Informed Consent
All animal procedures were approved by the Vanderbilt University IACUC (M1600225). All procedures performed in studies involving animals were in accordance with the ethical standards of the institution at which the studies were conducted. Welfare-related assessments were carried out prior to and throughout all experiments by trained personnel at Vanderbilt University and Vanderbilt University Medical Center. This article does not contain any studies with human participants performed by any of the authors.
Figures
References
-
- Garland DE (1988) Clinical observations on fractures and heterotopic ossification in the spinal cord and traumatic brain injured populations. Clin Orthop Relat Res (233):86–101 - PubMed
-
- Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J Bone Joint Surg Br. 2005;87(1):2–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
